Peter Nash discusses the latest evidence on the association between JAK inhibitors and the risk for VTE, MACE, and malignancy
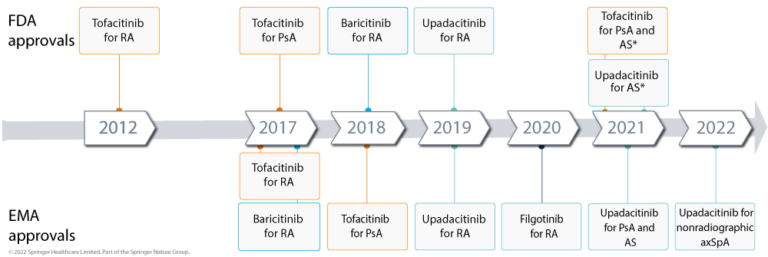
medwireNews: Janus kinase (JAK) inhibitors are the newest class of drugs for the treatment of rheumatoid arthritis (RA), with three JAK inhibitors now approved by the US FDA and four by the EMA (figure 1).
These oral agents offer a number of potential advantages for people with inflammatory arthritis, but some safety concerns have emerged, including a possible increased risk for venous thromboembolism (VTE), major adverse cardiovascular events (MACE), and malignancy.
Here we talk to Peter Nash, Professor and rheumatologist from Griffith University in Brisbane, Queensland, Australia, about the current understanding of these potential risks, in the context of the benefits they offer.
A popular treatment option
JAK inhibitors are “so popular” in many countries at present, with about 25% market share for RA in Australia, “including one in three patients who fail conventional DMARDs and one in three who fail or are intolerant of a biologic DMARD,” says Nash. He explains that there are a number of reasons for this, including their oral route of administration and short half-life, meaning that they can be stopped when needed, such as when adverse events occur or when a patient requires surgery or wishes for pregnancy.
“There’s no immunogenicity signal if you stop and start” JAK inhibitors, he adds.
Nash also notes that these agents can be used as monotherapy by people with an intolerance or contra-indication to methotrexate and they have “major generic potential,” which could provide “highly effective treatment to a huge number of people in need,” particularly those in impoverished Asia–Pacific settings.
All the JAK inhibitors have had “very comprehensive clinical trial programs,” remarks Nash, noting that they have shown either noninferiority or superiority to the gold standard treatment, “which has been adalimumab plus methotrexate for many, many years.”
For instance, the ORAL Strategy trial demonstrated noninferiority of the JAK1/3 inhibitor tofacitinib to adalimumab when given in combination with methotrexate, while RA-BEAM and SELECT-COMPARE showed that the JAK1/2 inhibitor baricitinib and the selective JAK1 inhibitor upadacitinib are “clearly superior to the gold standard,” Nash commented. “Interestingly, the difference [was] driven by pain, and patient and physician global assessment,” he noted.
“No one’s pretending that they don’t have issues, particularly [herpes] zoster,” but the JAK inhibitors have “a safety profile that’s been manageable,” he says.
Nash points out that two things have raised questions over JAK inhibitor safety, namely “the unresolved issue” of whether VTE risk is a class effect or linked to JAK2 inhibition only, and an announcement of preliminary results from the ORAL Surveillance study showing elevated rates of MACE and malignancy in RA patients treated with tofacitinib versus tumor necrosis factor (TNF) inhibitors.
VTE: A class effect?
VTE risk “first became an issue in the early days of the baricitinib studies, where there was a numerical increase in VTEs versus the comparators, particularly placebo,” Nash explains. A pooled safety analysis of data from nine phase 1–3 randomized controlled trials in RA found that six of 997 participants treated with baricitinib 4 mg/day experienced VTE events over 24 weeks, compared with none of 1070 given placebo. Nash notes, however, that this increase in VTE rates with baricitinib versus placebo “did not hold true in the long-term extension studies.”
Similarly, he says that there was an imbalance in VTE rates in one of the initial upadacitinib trials; in the 24-week SELECT-BEYOND trial there were a total of four adjudicated pulmonary embolism events in participants who were treated with upadacitinib 15 mg/day or 30 mg/day throughout the study or who switched from placebo to upadacitinib at week 12, compared with none in participants treated with placebo during weeks 1–12.
But again, when they did the SELECT-COMPARE trial, comparing upadacitinib 15 mg/day, placebo, and adalimumab on a background of methotrexate, VTE risk “was balanced across the groups,” adds Nash. In this study, adjudicated VTE rates were 0.3%, 0.2%, and 0.9% in the upadacitinib, placebo, and adalimumab groups, respectively. A pooled analysis of data from the SELECT trials also found no significant increase in VTE risk associated with upadacitinib.
Moreover, the preliminary results from the ORAL Surveillance study, comparing tofacitinib with TNF inhibitors in RA patients aged 50 years and older with at least one additional cardiovascular risk factor, also “did not show a VTE signal,” says Nash.
“And so, it remains unresolved: is VTE a JAK2 inhibition effect [as shown in one of] the initial baricitinib placebo trials, or is it a JAK class effect?” he speculates.
“There is not a lot of evidence for a class effect; [events were] seen in an early baricitinib study, and did not seem to be an issue at long-term follow-up,” but “maybe there is some selection bias” because “people at risk had dropped out,” or those at high risk were excluded from studies, summarizes Nash.
VTE: Practical considerations for rheumatologists
So what should rheumatologists do in light of these uncertainties?
Nash stresses that “VTE is associated with rheumatoid arthritis itself, particularly in the active, poorly controlled phase,” and therefore disease control is key.
“We don’t use JAK inhibitors in people who have a strong history of venous thromboses, [and] we don’t use them in people who are at high risk of VTE, like [those with] factor V Leiden deficiency,” he says. However, while other RA medications are more appropriate for people with a history of blood clots, he believes “that sometimes having failed every other therapy, [a JAK inhibitor is] still the right thing to choose.”
“You just have to weigh up risk and benefit in the individual.”
Nash notes that precautionary measures can be taken to reduce VTE risk in people taking JAK inhibitors, such as stopping treatment “for a few days” around the time of a long-haul flight or if someone is undergoing surgery.
“I don’t think there’s any data proving that this would change risk, but it seems quite a reasonable thing to do,” he says.
Are JAK inhibitors linked to MACE?
In addition to the currently unresolved VTE issue, the preliminary results from ORAL Surveillance also raise the question of whether JAK inhibitors are associated with MACE and malignancy risk, says Nash.
According to a press release, incidence rates for MACE in the ORAL Surveillance study were 0.98 per 100 person–years for RA patients treated with any dose of tofacitinib, compared with 0.73 per 100 person–years for those given a TNF inhibitor, giving a significant hazard ratio (HR) of 1.33.
“There was a difference in risk, but it was quite small,” with a number needed to harm of “nearly 600 patients treated for a year to get one extra case,” says Nash.
“That risk to me does not seem to be particularly high and you shouldn’t throw out a medication based on that particular risk,” he adds.
Nash emphasizes the importance of instead addressing traditional risk factors for MACE, including lipids, blood pressure, and smoking, as well as controlling RA disease activity.
A potential signal for malignancy
Turning to malignancy, Nash says that the ORAL Surveillance study showed a difference in rates of malignancy with tofacitinib versus TNF inhibitor. Specifically, adjudicated malignancy rates (excluding nonmelanoma skin cancer) were 1.13 per 100 person–years with any dose of tofacitinib, compared with 0.77 per 100 person–years with TNF inhibitors, resulting in a significant HR of 1.48.
“Rheumatoid [arthritis] is associated with lung cancer, [and] can be associated with lymphoma, so it’s more important to stop people smoking and turn off some of those other very important risk factors,” but “there is a small difference” in risk, says Nash. He adds that “278 patients had to be treated for a year to get one extra malignancy that was not skin.”
While the preliminary findings from ORAL Surveillance highlight potential risks, Nash cautions that “until we’ve seen the peer-reviewed paper, we can’t tell whether there was any baseline imbalance in either MACE risk factors or malignancy risk factors.
“If there were 30% less smokers in one group compared to the other, just by chance […] that might be enough to explain the difference” in these adverse events, he says.
Don’t throw the baby out with the bathwater
“The JAKs, I think, are here to stay – I think we have to learn how to use them wisely,” remarks Nash.
“The risk is that we’ll throw the baby out with the bathwater and lose a valuable group of medications on hearsay,” so “the sooner [the ORAL Surveillance results are published], the better for everybody.”
He recommends that future studies to better understand the risks associated with JAK inhibitors should include an investigation on whether JAK inhibitors affect levels of biomarkers for thrombogenic risk – such as factor V Leiden, anti-thrombin-3, and lupus anticoagulant – as well as research into “whether TNF inhibitors reduce MACE risk rather than tofacitinib increasing it” and how baseline risk factors influence malignancy risk.
“And we just have to be clever with how we use a very helpful class of drug, rather than throw our arms up.”
medwireNews is an independent medical news service provided by Springer Healthcare Ltd. © 2021 Springer Healthcare Ltd, part of the Springer Nature Group